4 mg/2 ml, 8 mg/4 ml
For the use of a Registered Medical Practitioner or a Hospital or a Institution only.
ONONE (Ondansetron HCl) is a racemic form of ondansetron and a selective blocking agent of the serotonin 5-HT3 receptor type. Chemically, Ondansetron HCl is 4H-Carbazol-4-one, 1,2,3,9-tetrahydro-9-methyl-3-(2-methyl-1H-imidazol-1-yl)methyl-, monohydrochloride,
(±)-, dihydrate. Its molecular formula is C18H19N3O·HCl·2H2O and its molecular weight is 365.86.
STRUCTURAL FORMULA :
Its structural formula is :
-STRUCUTRE.jpg)
ONONE is a clear, colourless solution filled in amber glass ampoule of suitable size.
COMPOSITION :
Each ml contains :Ondansetron Hydrochloride Dihydrate USP
equivalent to Ondansetron .............................2 mg
Water for Injection USP .....................................q.s.
ACTIONS :
Ondansetron is a potent, highly selective 5HT3 receptor-antagonist. Its precise mode of action in the control of nausea and vomiting is not known. Chemotherapeutic agents and radiotherapy may cause release of 5HT in the small intestine initiating a vomiting reflex by activating vagal afferents via 5HT3 receptors. Ondansetron blocks the initiation of this reflex. Activation of vagal afferents may also cause a release of 5HT in the area postrema, located on the floor of the fourth ventricle and this may also promote emesis through a central mechanism. Thus, the effect of ondansetron in the management of the nausea and vomiting induced by cytotoxic chemotherapy and radiotherapy is probably due to antagonism of 5HT3 receptors on neurons located both in the peripheral and central nervous system.
The mechanisms of action in post-operative nausea and vomiting are not known but there may be common pathways with cytotoxic induced nausea and vomiting. Ondansetron does not alter plasma prolactin concentrations. The role of ondansetron in opiate-induced emesis is not yet established.
PHARMACOKINETICS :
The disposition of ondansetron following oral, intramuscular (I.M.) and intravenous (I.V.) dosing is similar with a terminal half life of about 3 hours and steady state volume of distribution of about 160 L. Equivalent systemic exposure is achieved after I.M. and I.V. administration of ondansetron. Ondansetron is not highly protein bound (70 - 76 %). Ondansetron is cleared from the systemic circulation predominantly by hepatic metabolism through multiple enzymatic pathways. Less than 5 % of the absorbed dose is excreted unchanged in the urine. The absence of the enzyme CYP2D6 (the debrisoquine polymorphism) has no effect on ondansetrons pharmacokinetics. The pharmacokinetic properties of ondansetron are unchanged on repeat dosing. In a study of 21 paediatric patients aged between 3 and 12 years undergoing elective surgery with general anaesthesia, the absolute values for both the clearance and volume of distribution of ondansetron following a ingle intravenous dose of 2 mg (3 - 7 years old) or 4 mg (8 - 12 years old) were reduced. The magnitude of the change was age-related, with clearance falling from about 300 ml/min at 12 years of age to 100 ml/min at 3 years. Volume of distribution fell from about 75 L at 12 years to 17 L at 3 years. Use of weight-based dosing (0.1 mg/kg up to 4 mg maximum)
compensates for these changes and is effective in normalising systemic exposure in paediatric patients.
In patients with renal impairment (creatinine clearance 15 - 60 ml/min), both systemic clearance and volume of distribution are reduced following I.V. administration of ondansetron, resulting in a slight, but clinically insignificant, increase in elimination half-life (5.4 h). A study in patients with severe renal impairment who required regular haemodialysis (studied between dialyses) showed ondansetrons pharmacokinetics to be essentially unchanged following I.V. administratio. Specific studies in the elderly or patients with renal
impairment have been limited to I.V. and oral administration. However, it is anticipated that the half-life of ondansetron after rectal administration in these populations will be similar to that seen in healthy volunteers, since the rate of elimination of ondansetron following rectal administration is not determined by systemic clearance. Following oral, intravenous or intramuscular dosing in patients with severe hepatic impairment, ondansetrons systemic clearance is markedly reduced with prolonged elimination half-lives (15 - 32 h) and an oral bioavailability approaching 100 % due to reduced pre-systemic metabolism.
INDICATIONS :
1. Prevention of nausea and vomiting associated with initial and repeat courses of emetogenic cancer chemotherapy, including high dose of cisplatin. Efficacy of the 32 mg single dose beyond 24 hours in these patients has not yet been established.
2. Prevention of postoperative nausea and/or vomiting. As with any other antiemetic, routine prophylaxis is not recommended for patients in whom there is little expectation that nausea and/or vomiting will occur postoperatively. In patients where nausea and/
or vomiting must be avoided postoperatively ONONE Injection is recommended even where the incidence of post operative nausea and/or vomiting is low. For patients who have nausea and/or vomiting postoperatively, ONONE Injection may be given to prevent further episodes.
Administration :
FOR INTRAVENOUS AND INTRAMUSCULAR USE ONLY. ONONE is also available for oral use to allow the route of administration and dosing to the flexible.
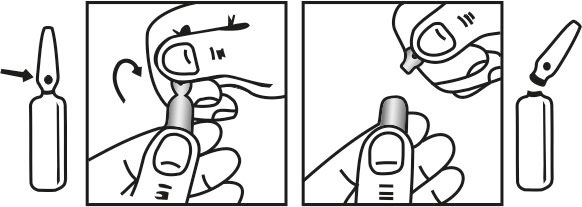
INSTRUCTION FOR USE OF AMPOULE :
The ampoule used in this product is equipped with O.P.C (One Point Cut) opening system. No ampoule file is needed to open the ampoule. The neck of the ampoule is prescored at the point of constriction. A coloured dot on the ampoule head helps to orientate the ampoule. Take the ampoule and face the coloured dot. Let the solution at the head of the ampoule to flow down by shaking or a gentle stroke. The ampoule opens easily by placing the thumb on the coloured dot and gently pressing downwards as shown.
Dosage :
Chemotherapy and radiotherapy :
Adults :
The emetogenic potential of cancer treatment varies according to the doses and combinations of chemotherapy and radiotherapy regimens used. The route of administration and dose of ONONE should be flexible in the range of 8 - 32 mg a day and selected as shown below.
Emetogenic chemotherapy and radiotherapy :
ONONE can be given either by rectal, oral (tablets or syrup), intravenous or intramuscular administration. For most patients receiving emetogenic chemotherapy or radiotherapy, ONONE 8 mg should be administered as a slow intravenous or intramuscular injection immediately before treatment, followed by 8 mg orally 12 hourly. To protect against delayed or prolonged emesis after the first 24 hours, oral or rectal treatment with ONONE should be continued for up to 5 days after a course of treatment.
Highly emetogenic chemotherapy :
For patients receiving highly emetogenic chemotherapy, e.g. high-dose cisplatin, ONONE can be given either by rectal, intravenous or intramuscular administration. ONONE has been shown to be equally effective in the following dose schedules over the first 24 hours of chemotherapy :
A single dose of 8 mg by slow intravenous or intramuscular injection immediately before chemotherapy. A dose of 8 mg by slow intravenous or intramuscular injection immediately before chemotherapy, followed by two further intravenous or intramuscular doses of 8 mg 2 to 4 hours apart, or by a constant infusion of 1 mg/hour for up to 24 hours. A single dose of 32 mg diluted in 50 - 100 ml of saline or other compatible infusion fluid and infused over not less than 15 minutes immediately before chemotherapy. The selection of dose regimen should be determined by the severity of the emetogenic challenge. The efficacy of ONONE in highly emetogenic chemotherapy may be enhanced by the addition of a single intravenous dose of dexamethasone sodium phosphate, 20 mg administered prior to chemotherapy. To protect against delaye or prolonged emesis after the first 24 hours, oral or rectal treatment with ONONE should be continued for up to 5 days after a course of treatment.
Children :
ONONE may be administered as a single intravenous dose of 5 mg/m2 immediately before chemotherapy, followed by 4 mg orally 12 hours later. 4 mg orally twice daily should be continued for up to 5 days after a course of treatment. Post-operative nausea and vomiting (PONV) :
Adults :
For the prevention of Post-operative nausea and vomiting ONONE can be administered orally or by intravenous or intramuscular injection. ONONE may be administered as a single dose of 4 mg given by intramuscular or slow intravenous injection at induction of anaesthesia. For treatment of established Post-operative nausea and vomiting a single dose of 4 mg given by intramuscular or slow intravenous injection is recommended.
Children (aged 2 years and over) :
For prevention of Post-operative nausea and vomiting in paediatric patients having surgery performed under general anaesthesia, ondansetron may be administered by slow intravenous injection at a dose of 0.1 mg/kg up to a maximum of 4 mg either prior to, at or after induction of anaesthesia. For treatment of established Post-operative nausea and vomiting in paediatric patients, ondansetron may be administered by slow intravenous injection at a dose of 0.1 mg/kg up to a maximum of 4 mg.
COMPATIBILITY AND STABILITY :
Impatibility with intravenous fluids. ONONE Injection should only be admixed with those infusion solutions which are recommended : Sodium Chloride Injection USP 0.9 % w/v Dextrose Injection USP 5 % w/v Mannitol Injection USP 10 % w/v Ringers Injection USP
Ringers and Dextrose Injection USP In keeping with good pharmaceutical practice dilutions of ONONE Injection in intravenous fluids should be prepared at the time of infusion and any remaining solution should be discarded. Compatibility studies have been undertaken in polyvinyl chloride infusion bags and polyvinyl chloride administration sets. It is considered that adequate stability would also be conferred by the use of polyethylene infusion bags or Type I glass bottles. Dilutions of ONONE in sodium chloride 0.9 % w/v or in dextrose 5 % w/v have been demonstrated to be stable in polypropylene syringes. It is considered that ONONE Injection diluted with other compatible infusion fluids would be stable in polypropylene syringes.
COMPATIBILITY WITH OTHER DRUGS :
ONONE may be administered by intravenous infusion at 1 mg/hour, e.g. from an infusion bag or syringe pump. The following drugs may be administered via the Y-site of the ONONE giving set for ondansetron concentrations of 16 to 160 mcg/ml (e.g. 8 mg/500 ml and 8 mg/50 ml respectively).
Cisplatin : Concentrations up to 0.48 mg/ml (e.g. 240 mg in 500 ml) administered over 1 to 8 hours.
5 -Fluorouracil : Concentrations up to 0.8 mg/ml (e.g. 2.4 g in 3 litres or 400 mg in 500 ml) administered at a rate of at least 20 ml per hour (500 ml per 24 hours). Higher concentrations of 5-Fluorouracil may cause precipitation of ondansetron. The 5-Fluorouracil infusion may contain up to 0.045 % w/v magnesium chloride in addition to other excipients shown to be compatible.
Carboplatin : Concentrations in the range 0.18 mg/ml to 9.9 mg/ml (e.g. 90 mg in 500 ml to 990 mg in 100 ml), administered over 10 minutes to 1 hour.
Etoposide : Concentrations in the range 0.14 mg/ml to 0.25 mg/ml (e.g. 72 mg in 500 ml to 250 mg in 1 litre), administered over 30 minutes to 1 hour.
Ceftazidime : Doses in the range 250 mg to 2000 mg reconstituted with Water for Injection USP as recommended by the manufacturer (e.g. 2.5 ml for 250 mg and 10 ml for 2 g ceftazidime) and given as an intravenous bolus injection over approximately 5 minutes.
Cyclophosphamide : Doses in the range 100 mg to 1 g, reconstituted with Water for Injection USP, 5 ml per 100 mg cyclophosphamide, as recommended by the manufacturer and given as an intravenous bolus injection over approximately 5 minutes.
Doxorubicin : Doses in the range 10 - 100 mg reconstituted with Water for Injection USP, 5 ml per 10 mg doxorubicin, as recommended by the manufacturer and given as an intravenous bolus injection over approximately 5 minutes.
Dexamethasone : Dexamethasone sodium phosphate 20 mg may be administered as a slow intravenous injection over 2 - 5 minutes via the Y-site of an infusion set delivering 8 or 32 mg of ondansetron diluted in 50 - 100 ml of a compatible infusion fluid over approximately 15 minutes. Compatibility between dexamethasone sodium phosphate and ondansetron has been demonstrated supporting administration of these drugs through the same giving set resulting in concentrations in line of 32 mcg - 2.5 mg/ml for dexamethasone sodium phosphate and 8 mcg - 1 mg/ml for ondansetron.
-TABLE.jpg)