250 mg/5 ml
For the use of a Registered Medical Practitioner or a Hospital or a Institution only.
EPINOTIN (Phenytoin sodium) is a hydantoin derivative anticonvulsant. The chemical name is 2,4- Imidazolidinedione,5,5-diphenyl-, monosodium salt. The molecular formula is C15H11N2NaO2 and molecular weight is 274.3.
STRUCTURAL FORMULA :
Its structural formula is :
-Structure.jpg)
EPINOTIN is a clear, colourless solution filled in suitable size amber ampoule.
COMPOSITION :
Each ml contains :
Phenytoin Sodium I.P. 50 mg
Propylene Glycol I.P. 40 % v/v
Ethanol I.P. 10 % v/v
Water for Injections I.P. q.s.
ACTIONS :
Phenytoin sodium inhibits the spread of seizure activity in the motor cortex. It appears that by promoting sodium efflux from neurons, phenytoin sodium tends to stabilise the threshold against hyperexcitability caused by environmental changes or excessive stimulation capable of reducing membrane sodium gradient. This includes the reduction of post tetanic potentiation of synapses. Loss of post tetanic potentiation prevents cortical seizure foci from detonating adjacent cortical areas. Phenytoin thereby reduces the over-activity of brain stem centres responsible for the tonic phase of grand mal seizures. Phenytoin sodium’s antiarrhythmic action may be attributed to the normalization of influx of sodium and calcium to cardiac Purkinje fibres. Abnormal ventricular automaticity and membrane responsiveness are decreased. It also shortens the refractory period, and therefore shortens the QT interval and the duration of the action potential. Hydantoins induce production of liver microsomal enzymes, thereby accelerating the metabolism of concomitantly administered drugs.
PHARMACOKINETICS :
The onset of action after an intravenous dose is 30 to 60 minutes and the effect persists up to 24 hours. Phenytoin is about 90 % protein bound. Protein binding may be lower in neonates and hyperbilirubinaemic infants; also altered in patients with hypoalbuminaemia, uraemia or acute trauma, and in pregnancy. Optimum control without clinical signs of toxicity occurs most often with serum levels between 10 and 20 µg/ml. In renal failure or hypoalbuminaemia, 5 to 12 µg/ml or even less may be therapeutic. Phenytoin is metabolised in the liver, the major inactive metabolite is 5-(p-hydroxyphenyl)-5-phenylhydantoin (HPPH). The rate of metabolism is increased in younger children, pregnant women, in women during menses and in patients with acute trauma. The rate decreases with advancing age. Phenytoin may be metabolised slowly in a small number of individuals due to genetic factors, which may cause limited enzyme availability and lack of induction. The plasma half-life is normally from 10 to 15 hours. Because phenytoin exhibits saturable or dose-dependent pharmacokinetics, the apparent half-life of phenytoin changes with dose and serum concentration. At therapeutic concentrations of the drug, the enzyme system responsible for metabolising phenytoin becomes saturated. Thus a constant amount of drug is metabolised, and small increases in dose may cause disproportionately large increases in serum concentrations and apparent half-life, possibly causing unexpected toxicity.
INDICATIONS :
For the control of status epilepticus of the grand mal type and the prevention of seizures occurring during or following neurosurgery. It has also been used in the treatment of certain cardiac arrhythmias, particularly in those patients who do not respond to conventional antiarrhythmic agents or to cardioversion.
Administration :
EPINOTIN must be administered slowly Intravenous administration should not exceed 50 mg/minute in adults. In neonates the drug should be administered at a rate not exceeding 1 to 3 mg/kg/min. Dilution of EPINOTIN into intravenous infusion is not recommended due to lack of solubility and resultant precipitation. EPINOTIN should be injected slowly and directly into a large vein through a large-gauge needle or intravenous catheter. Each injection should be followed by an injection of sodium chloride intravenous infusion 0.9 % through the same needle or catheter to avoid local venous irritation due to the alkalinity of the solution. Continuous infusion should be avoided.
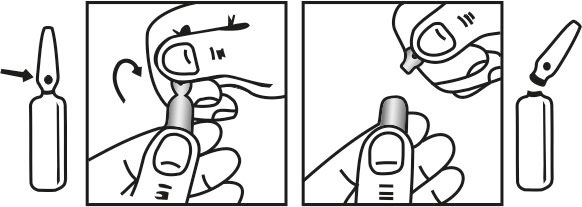
INSTRUCTIONS FOR USE OF AMPOULE :
The ampoule used in this product is equipped with O.P.C (One Point Cut) opening system. No ampoule file is needed to open the ampoule. The neck of the ampoule is prescored at the point of constriction. A coloured dot on the ampoule head helps to orientate the ampoule. Take the ampoule and face the coloured dot. Let the solution at the head of the ampoule to flow down by shaking or a gentle stroke. The ampoule opens easily by placing the thumb on the coloured dot and gently pressing downwards as shown.
Dosage :
For the control of status epilepticus in adults, a loading dose of 10 to 15 mg/kg should be administered slowly intravenously, at a rate not exceeding 50 mg/minute. The loading dose should be followed by maintenance doses of 100 mg orally or intravenously every 6 to 8 hours. For neonates and children a loading dose of 10 to 20 mg/kg intravenously will usually provide a plasma concentration of phenytoin within the generally accepted therapeutic range (10 to 20 micrograms/ml). The drug should be administered intravenously at a rate not exceeding 1 to 3 mg/kg/min. In the treatment of status epilepticus an intravenous benzodiazepine such as diazepam is usually given initially for the rapid control of seizures and is then followed by the slow intravenous administration of phenytoin. Intramuscular administration of phenytoin is unsuitable for the emergency treatment of status epilepticus due to very slow and erratic absorption from the intramuscular site. For the prevention of seizures during or following neurosurgery, cautious intravenous administration of 250 mg every six to twelve hours is recommended until oral dosage is possible. Plasma levels should be monitored to ensure optimal efficacy and to minimise toxicity. Phenytoin should not be given by intramuscular injection for the prevention of seizures following neurosurgery.
Phenytoin sodium can be useful in ventricular arrhythmias. Although not a cardiac depressant, it has a positive inotropic effect and enhances conduction, though it generally decreases automaticity. The recommended dosage is one intravenous injection of EPINOTIN of 3 to 5 mg/kg bodyweight initially, repeating if necessary.
CONTRAINDICATIONS :
1. Patients with a known hypersensitivity to phenytoin or other hydantoins.
2. Patients with sinus bradycardia, sino-atrial block, second and third degree AV block or Adams-Stokes syndrome.
3. Intra-arterial administration must be avoided in view of the high pH of the preparation.
WARNINGS :
This drug must be administered slowly, at a rate not exceeding 50 mg/minute in adults. In neonates, the drug should be administered at a rate not exceeding 1-3 mg/kg/min. The response to phenytoin may be significantly altered by the concomitant use of other drugs (see Interactions). In patients with cardiovascular disease, parenteral administration may result in atrial and ventricular conduction depression, ventricular fibrillation or reduced cardiac output. Severe complications are most commonly encountered in elderly or gravely ill patients. In these patients, the drug should be administered at a rate not exceeding 25 mg/minute, and if necessary, at a slow rate of 5 to 10 mg/minute. The intramuscular administration of phenytoin sodium is not recommended due to erratic absorption and local tissue reactions when given by this route. Phenytoin should be used with caution in diabetic patients, as hyperglycaemia may be potentiated. Patients with renal function impairment should be carefully observed when prescribing phenytoin, as excretion and protein binding may be altered. Similarly, because phenytoin is metabolised in the liver, dosage reduction may be required in patients with extensive hepatic impairment. Abrupt withdrawal of phenytoin in epileptic patients may precipitate status epilepticus. When the need arises for a dosage reduction of phenytoin, or discontinuation or substitution of alternative anticonvulsant therapy is required, this should be done gradually. In hypersensitivity reactions, where rapid substitution of therapy is warranted, the alternative drug should be one not belonging to the hydantoin class of compounds. Phenytoin should be used with caution in patients with hypotension and severe myocardial insufficiency. Caution should also be used when administering phenytoin to patients suffering from porphyria. There have been isolated reports linking phenytoin to exacerbation of this disease. Hypotension usually occurs when the drug is administered rapidly by the I.V. route.
PRECAUTIONS :
Soft tissue irritation and inflammation, varying from slight tenderness to extensive necrosis and sloughing, has been noted at the site of injection. Each injection of phenytoin should be followed by an injection of sodium chloride intravenous infusion 0.9 % through the same needle or catheter to avoid the irritation. The liver is the principal site of biotransformation of phenytoin; patients with impaired liver function, elderly patients, or those who are gravely ill may show early signs of toxicity. A small percentage of individuals who have been treated with phenytoin have been shown to metabolize the drug slowly. Slow metabolism appears to be due to limited enzyme availability and lack of induction, which may be genetically determined. There have been a number of reports suggesting a relationship between phenytoin and the development of local or generalised lymphadenopathy, including benign lymph node hyperplasia, lymphoma, pseudolymphoma and Hodgkin’s Disease. Although a cause and effect relationship has not been established, the occurrence of lymphadenopathy requires differentiation from other types of lymph node pathology. Lymph node involvement may occur with or without symptoms resembling serum sickness e.g. rash, fever and liver involvement. In all cases of lymphadenopathy, seizure control should be sought
using alternative antiepileptic drugs and observation of patients for an extended period is recommended. Serum levels of phenytoin sustained above the optimal range may produce encephalopathy, or confusional states (delirium psychosis), or rarely irreversible cerebellar dysfunction. Plasma level determinations are recommended at the first signs of acute toxicity. If plasma levels are excessive, then dosage reduction is indicated. Termination is recommended if symptoms persist (see Warnings). Phenytoin should be discontinued if a skin rash appears. If the rash is exfoliative, purpuric, or bullous or if lupus erythematosus, Stevens-Johnson syndrome or toxic epidermal necrolysis is suspected, phenytoin should not be resumed. If the rash is mild (measles-like or scarlatiniform), resumption of therapy will depend on a consideration of the risk/benefit ratio by the treating physician. However, in the case of the rash recurring upon reinstitution of therapy, further phenytoin medication is contraindicated. Phenytoin is not effective for petit mal seizures. Therefore, combined therapy is required if both grand mal and petit mal seizures are present. There have been isolated reports of hyperglycaemia occurring in patients receiving phenytoin, resulting from the drug’s inhibition of insulin secretion. Phenytoin may also raise the serum glucose in diabetic patients.
Pregnancy : Pregnancy Category D.
-Table.jpg)